AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2768-0487/031
1Specialist general surgery and lecturer general surgery Dubai Medical College Dubai UAE.
2Specialist internal medicine Dubai hospital, UAE.
3Assistant Professor GI department SIUT.
4Medical officer Sindh children services hospital.
5Associate professor GI department SIUT.
6Senior specialist general surgery Dubai Hospital UAE.
7Consultant general surgeon, Liaquat National Hospital Karachi Pakistan.
8Consultant and head of general’s surgery department LiAQUAT National hospital Karcahi, Pakistan.
*Corresponding Author: Aliya Ishaq, Specialist general surgery and lecturer general surgery Dubai Medical College Dubai UAE.
Citation: A Ishaq, MJH Khan, Muhammad s khan, M Ishaq, A Parveen, et al. (2021) Enterocutaneous fistula; Management challenges, Areterospective review of 11 patients treated in our institute. Journal of Clinical and Laboratory Research. 3(1); DOI:10.31579/2768-0487/031
Copyright: ©2021 Aliya Ishaq. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 June 2021 | Accepted: 11 June 2021 | Published: 16 June 2021
Keywords: enterocutaneous fistula; enteroatmospheric fistula; spontaneous closure; mortality; timeline
Enterocutaneous fistula is a local pathology and systemic disorder.
OBJECTIVES:
To analyze postoperative outcomes, morbidity, and mortality in patients treated for enterocutaneous fistula in our institute for past 18 months.
DESIGN, SETINGS AND PATIENTS:
Reterospective review of records of patients presented to Liaquat national university hospital Karachi, Pakistan between Jan 2010 to June 2011 with diagnosis of EC fistula.
RESULTS:
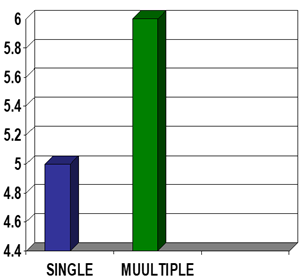
A total of eleven patients presented with diagnosis of enterocutaneous fistula in our institute in specified duration. Mean age at presentation was 33 years with amle to female ratio of 3:1.72.7 % had high output fistula and 27.2 % had low output fistula. Small bowel was involved in 72.7%, large bowel in 18.18% and 9.0% had both small and large bowel fistula.45.45% patients had single fistula while 54.55 had multiple fistula. Total length of stay varied between 22-150 days .6/11 (54.54%) had nosocomial infection, 3/11(27.27%) had bed sores.2/11(18.18%) had TPN related complications.Spontaneous closure occurred in 8/11(72.77) patients and definitive surgical closure was performed in one patient. Mortality rate was 18.8 %.
CONCLUSION:
Enterocutaneous fistula is a devastating outcome for both surgeons and patients, sytemetic timely multidisciplinary approach can save lives.
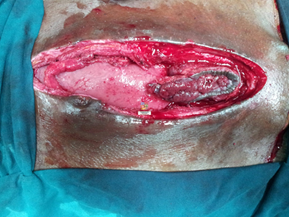
An enterocutaneous fistula (ECF) is an abnormal connection between the gastrointestinal tract and the skin or atmosphere (enteroatmospheric fistula [1] [EAF]) .Estimated 75-85% are iatrogenic, occur after an abdominal surgery.
There are several ways in which ECF has been classified, including by output, etiology, and source [1, 2, 3]. Most often, a high-output ECF is characterized as one with >500 mL/24 hours, low output <200 mL/24 hours, and a moderate output fistula between 200 and 500 mL/24 hours [1].
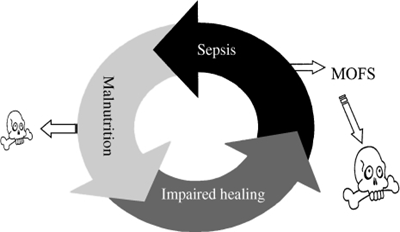
Historical reported mortality rates as high as 10-30%. Sepsis is the leading cause of death. Other factor include high output and comorbidity.Recent reported series show a declining mortality (6-33 or less) with improving supportive care, especially nutrition [3].
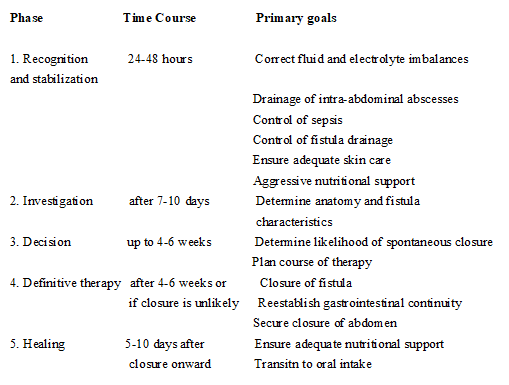
There is consensus among authorities that the management of a patient with EC fistula should proceed in an ordered sequence [3].
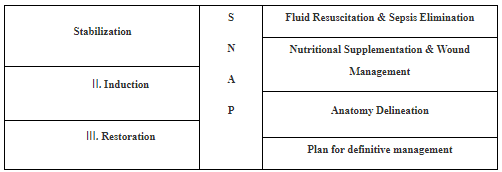
Treatment phases [4]
Management:
Management can be divided in to three phases
Acute phase:
Window period:
Subacute phase:
Repair and reconstructive phase:
OBJECTIVE:
INCLUSION CRITERIA:
All patients who presented to hospital with enterocutaneous fistula for previous 2 years were included in study.
They were all primarily treated in peripheral hospitals.
Management:
We adopted the three phase approach as described above for management of all patients with ECF (entero cutaneous fistula)
In the first phase (the acute phase) recognition and stabilization of ec fistula was done. The goal of this phase was to correct fluid and electrolyte imbalances, malnutrition, sepsis,abscess formation and wound infection. These problems were addressed within first 24-48 hrs of admission.
DVT prophylaxis.
The next phase was phase of anatomical delieniation.
Other had multiple fistulae in both small and large gut (post gun shot, multiple laparotomies.
Different ways used for enteral feeding. For all low output and distal fistulas enteral feeding was started immediately after delineation and predigested dietary supplements were uses. In two patients with high output proximal fistula fistuloclysis was tried that is fistula contents taken from proximal limb through a feeding tube and reinserted distally using a Foley catheter and balloon inflated with 15 ml of water, It was very difficult and messy and was not totally successful requiring loss as well as multiple time cleaning because of leakage but was continued.
One patient feeding jejunostomy was made during initial surgery while controlling the sepsis and was used for enteral feeding.
Different types of dressings and drains were used to prevent skin complications related to fistula



DRESSINGS USED:
In the final phase, definitive operation was done including fistula resection and resection anastomosis and biological mesh was used to reconstruct abdominal wall (one patient)
(Range: 15 - 45)
Type of fistula:
High output: 72.7%
Low output: 27.2%

Location of fistula:
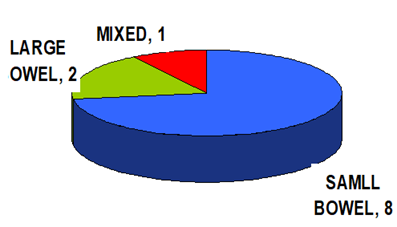
No of fistulae:

Except for 3 patient all presented with sepsis and were nutritionally depleted.
Morbidity:
Recurrence: 1 out of 2 in surgically treated patient
Readmissions: 1
Length of hospital stay: 22 – 150 days.
Nosocomial infections: 6
Bed sore: 3
TPN related complications: 2
Line sepsis: 2
CVP Line: Out of 6, 2 had sepsis
PICC Line: Out of 5 none had sepsis
Mortality: 2 (18.18%)
Cause of mortality include multiple proximal high output fistulae and severe sepsis.
Spontaneous closure: 8 out of 11(72.7%) in 20 days to 3 months period.
Defenitive procedure after sub-acute phase: 1 out of 11 after 6 months of conservative treatment.
Patients died in sub-acute phase: 2 out of 11
The enterocutaneous fistula (ECF) is a devastating complication for both surgeons and patients alike. Prior to the advent of sophisticated critical care support and parenteral nutrition, the development of an ECF nearly equated to a death sentence. In the current era, the mortality rate has been reduced to 5 to 20% [5, 6]. However, the development and management of an ECF remains a chronic, debilitating condition [5].
We used the standard approach described by Schecter et al [6] for the management of EC fistula that is divided in 3 phases,first phase includes recognition and stabilization ,so patients after being diagnosed with having EC fistula were admitted in high dependency unit and correction of electrolytes and fluid balances were done along with control of fistula and sepsis source control. Patients with severe sepsis underwent ct scan abdomen with contrast in initial phase and those having intrabdominal collection and sepsis were taken to operation theater and drainage of abcess with controleed fistula formation was done as well as feeding jejunostomy was made in 2 cases, specialized vacuum dressings with laparostomy and vicryl mesh placement in presence of controlled fistula was performed in 2 patients. Broad spectrum antibiotics were started as per pus culture and blood transfusion was started when indicated. Parenteral nutrition was started in almost all patients and few of them with low output fistula were started on enteral feeding as well. Daily electrolytes and weight measurements were taken and strict in put out put charting was done along with chest and body physio and DVT prophylaxis
The provision of total parenteral nutrition has been associated with an increased rate of spontaneous closure of fistulas in several series [9, 10, 11]. Parenteral nutrition has long been recognized to be an integral part of the management of enterocutaneous fistulas [9, 10].We started TPN in all patients after insertion of PICC line /central line in acute phase. We don’t have enough number of patients to determine that correlation.
After 7 to 10 days, the patient has generally stabilized, and the fistula has matured to the point of supporting intubation of thin catheters in all orifices. At this point, the patient should undergo fluoroscopic fistulography with water-soluble contrast under the direct supervision of a senior radiologist and the senior surgeon responsible for the patient’s care. The information gained by such a study includes (1) the source of the fistula; (2) the nature (length, course, and relationships) of the fistula tract; (3) the absence or presence of bowel continuity (end vs. side fistula); (4) the absence or presence of distal obstruction; (5) the nature of the bowel adjacent to the fistula (inflammation, stricture); and (6) the absence or presence of an abscess cavity in communication with the fistula. The fistulogram provides information not obtainable through any other study, and early films can be particularly useful in defining anatomy and relationships. As previously discussed, water-soluble contrast may also be injected into abscesses at the time of drainage as a type of early fistulogram [9]. In our study. After the phase of stabilization and defining fistula output fistulogram was done to delineate the site of fistula and bowel anatomy and then same management with dressings ,TPN ,enteral feeding ,different dressings ,wound and skin care using zinc oxide was continued including fistuloclysis and patients were observed for a period of 3- 6 months .
We did not have a large enough sample to determine which factors determine good outcomes for enterocutaneous fistulas. However, several studies from other centers have looked at this. Using multiple logistic regression analysis, Visschers et al [15]. Found that intact abdominal walls and administration of parenteral nutrition were independent predictors of spontaneous closure of enterocutaneous fistulas. In our study Spontaneous closure was achieved in 3 months in 72.7 % cases without need for surgery and surgical intervention was done in 1 patient after completing 6 months of conservative treatment with mature fistula and repeat imaging using ct scan and fistulogram was done prior to surgery and excision of fistula followed by reconstructiuon and diversion ileostomy and abdominal wall reconstruction was done. 2 of our patients died in sub-acute phase because of hight output fistula and sever sepsis .Our mortality rate is 18.8% which is comparable to most institutes specialized in management of ECF.
Enterocutaneous fistula is a local pathology and systemic disorder with major impact on patient’s psychology,finance emotions and wellbeing . Given that most are iatrogenic, the most effective means of treatment is prevention with sound surgical judgment and meticulous technique. However, when faced with the development of an ECF, early recognition with systemic orderly approach by a multidisciplinary team specialized in treatment of these challenging patients can save lives.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
